











































Theory and Practice of Social Norms Interventions: Eight Common Pitfalls
London School of Hygiene and Tropical Medicine (Cislaghi); Johns Hopkins Bloomberg School of Public Health and School of Nursing (Heise)
"Awareness of these pitfalls has helped several programmes in the past increase the effectiveness of their interventions."
Many interventions in low- and middle-income countries (LMICs) aim to change social norms that sustain harmful practices, such as child marriage, female genital cutting, and intimate partner violence (IPV). However, when practitioners first apply a social norms frame to behaviour change, they may make mistakes. This paper outlines eight common pitfalls encountered when integrating a social norms perspective, as well as eight learnings.
The paper begins by reviewing some of the extensive and multi-disciplinary literature on social norms. For example, Cislaghi (2017, 2018) identified three steps for social norms change: (i) motivation (where participants learn about the detrimental consequences for themselves and others of their compliance with the harmful norm); (ii) deliberation (where participants create a new positive norm within their reference group and identify strategies to motivate others in their surroundings); and (iii) action (where participants publicly enact their strategies and motivate others to join the group, eventually reaching the critical mass needed for normative change).
The eight learnings, which correspond to the pitfalls, are:
- Social norms and attitudes are different: These two psychological constructs are connected but distinct (social norms can influence attitudes and vice versa). Attitudes are internally-motivated judgements that people make about something, whereas social norms are beliefs about what other people do and approve of. The misalignment between attitude and norm can influence the actions of multiple people in a group - e.g., everyone in a group might hold the attitude "I believe that girls should be at least 18 before they marry" but think that everyone else holds a different position ("the people around me marry their daughters as soon as they reach puberty, and expect me to do likewise"). This phenomenon is referred to as pluralistic ignorance. "Practitioners who implement an intervention to change social norms should pay attention to the difference between norms and attitudes as they design their measurement strategies, and select some of the tools created specifically to measure social norms."
- Social norms and attitudes can coincide: It is a mistake to focus exclusively on discordance between attitudes and norms. While correcting misperceptions might be an appropriate strategy when norms and attitudes are discordant, when people's attitudes align with the norm, practitioners may first need to change the attitudes of a core group of individuals and then help them become local change agents who can reach out to the larger group. "In sum, even though there is no universal relationship between attitudes and norms (either may change first), the two nonetheless influence each other in ways that practitioners should study and take account of in their work."
- Protective norms can offer important resources for achieving effective social improvement in people's health-related practices: An implicit bias in development is to see "culture" only as a source of problems rather than as a space for possible solutions. As an example, in some settings (e.g., Muslim-majority populations), a norm exists among adolescents under which drinking alcohol is considered a sign of weakness. "Effective interventions might work with local populations in devising strategies to strengthen protective norms, building on existing cultural values and worldviews..."
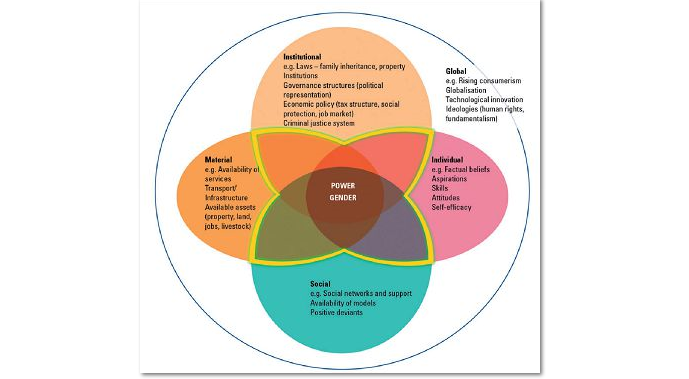
- Harmful practices are sustained by a matrix of factors that need to be understood in their interactions: Rather than assuming social norms are the sole driver of harmful practices, practitioners are advised to understand how norms intersect with other factors in order to uncover the pathways that motivate people to compliance with harmful practices. Norms against young female students' use of health services could be a possible barrier, but focusing on norms alone would be inadequate: The services themselves must exist and be accessible, and women need to know what services are offered and when they can access them. The figure above shows "a practical framework practitioners can use to look at that the ecology of factors contributing to sustaining any given practice..., which evolves from the well-known ecological framework....Understanding how institutional, individual, social and material factors interact to influence people’s harmful practices can help practitioners design effective interventions that include a social norms perspective."
- The prevalence of a norm is not necessarily a sign of its strength: "However, most studies thus far have invested more time, thought, and resources in measuring the prevalence of a norm (i.e. how many people in a specific group hold normative belief X), than measuring its influence (i.e. how many people do X because of the social norm)....Understanding the influence of one or multiple norms over a given practice should be a priority for effective intervention design. This could be done through qualitative research (see below), possibly coupled with quantitative measures ..."
- Social norms can exert both direct and indirect influence: Practitioners often study situations where the norm and the behaviour are matched (a direct relation), but a practice can also be indirectly sustained by multiple norms. IPV, for instance, might be sustained by the norms: "you're not supposed to intervene in another family's affairs"; "women are not supposed to disclose family matters to others"; and "women are supposed to keep the family together at any cost". Vignettes are one technique for diagnosing social norms' influence, but they "don't easily allow participants to deviate from the scenario that researchers present to them...; [o]pen-ended techniques are often better suited to situations where little is known about the norms that sustain a given practice. These methods might include participatory approaches that invite participants to discuss all possible contextual elements of the practice of interest."
- Publicising the prevalence of a harmful practice can make things worse: "[S]erious thought should be given to whether it will be beneficial to use messages that raise awareness in the general population of the size of a problem, like: '65,000 12-year-old girls were married this year in this region alone'. We don't yet know who is most likely to be influenced by such messages. It might be that these messages sway those who already hold personal attitudes in favour of the harmful practice; but a concrete risk exists that similar messages might backfire, pushing some previous non-compliers to comply with the harmful norm..."
- People-led social norm change is both the right and the smart thing to do: "Local worldviews, norms and attitudes intertwine to sustain cultural practices in ways that may be difficult for practitioners to fully decipher in culturally unfamiliar contexts. It can thus be dangerous to design a new desired system of norms from the “outside”. The consequences of the new normative equilibrium might be as harmful as the practices it is meant to replace. Practitioners should thus strive to design people-led interventions that help participants develop both internal motivations to change local norms and strategies to do so in ways that are compatible with the local cultural and social context..."
On December 18 2018, one of the authors, Beniamino Cislaghi, led a webinar discussing the paper; click the video below to view it.
Globalization and Health (2018) 14:83 https://doi.org/10.1186/s12992-018-0398-x; and STRIVE website, May 7 2021.
- Log in to post comments